The basic amenities many of us take for granted – heating, plumbing, phone service, and full kitchens – are not accessible to everyone. There are occupied homes in Southeastern Michigan that lack one or more of these amenities. While a majority of occupied homes throughout the region do have a heating source, indoor plumbing, phone service, and a full kitchen, the maps below show that the communities with the highest percentage of homes that lack such amenities are typically located in the more rural and urban areas of the region, not suburban areas.
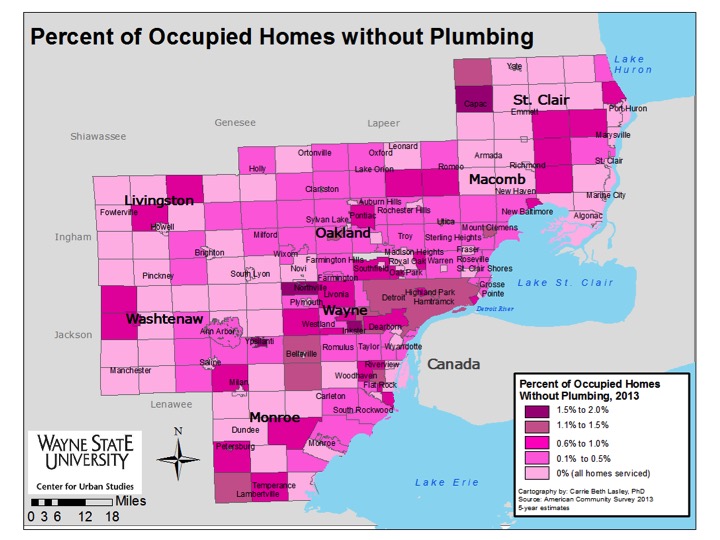
In Southeastern Michigan in 2013, there were only two communities, Inkster (1.5 percent) and Northville Township (1.8 percent), where between 1.5 and 2 percent of occupied homes were without complete plumbing (lacking either a toilet, a bathtub or shower, and/or running water). At a national level, about 1.6 million people are without complete indoor plumbing, according to a 2014 Washington Post article.
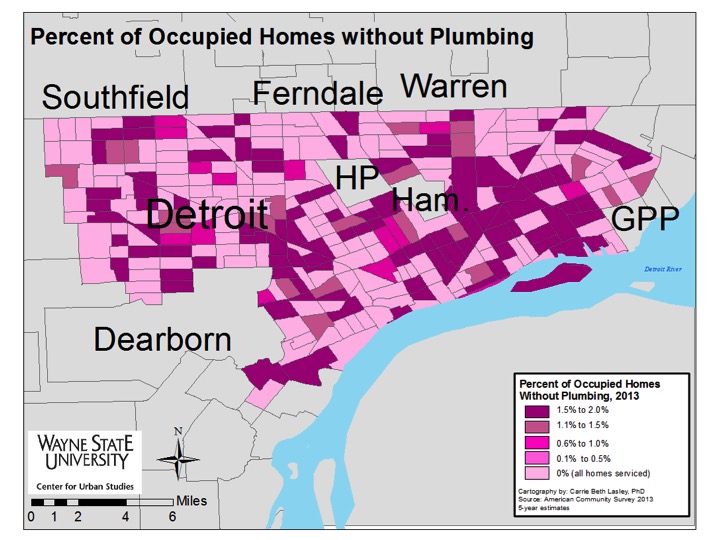
In 2013, 1.2 percent of the occupied homes in the city of Detroit were without complete plumbing facilities and this equated to 93 different census tracts in the city having homes without some type of complete plumbing facility. According to a 2013 post titled “Still Living without the Basics in the 21st Century” from the Rural Community Assistance Partnership, those living in densely populated urban areas and sparsely populated rural communities are more likely to live in a home without complete plumbing facilities, particularly if they live below the federal poverty level. In a post earlier this year, we detailed how a majority of the census tracts in the city of Detroit in 2013 had 50 percent or more of its children living below the poverty line. We also know that the median income in the city was $26,325 in 2013, which fell $26,721 below the national median income.
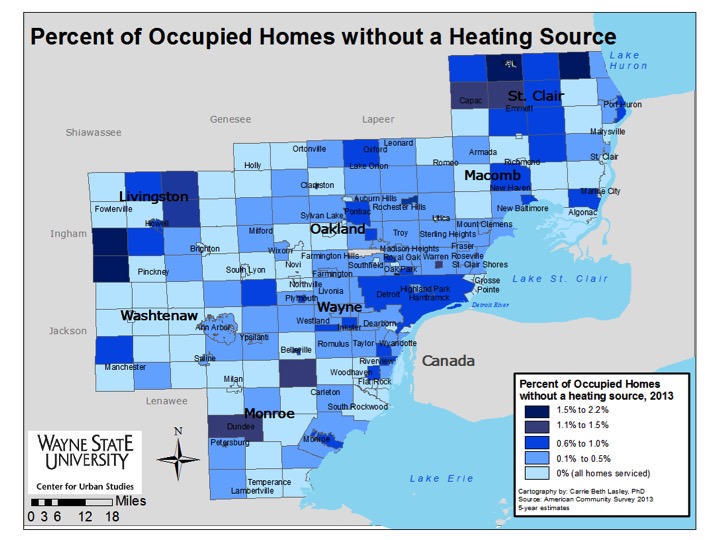
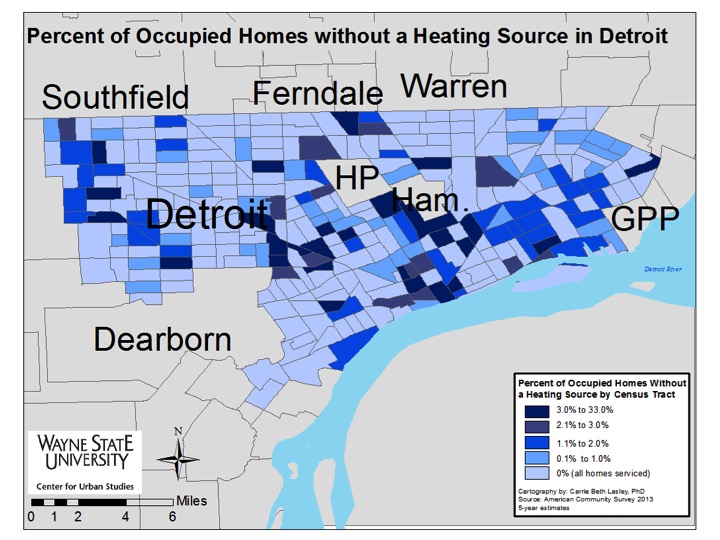
In Southeastern Michigan, the highest percentage of occupied homes without a heating source, meaning they lack heating equipment, were located in the rural communities on the outskirts of the region. In total, there were four communities in the region (two in St. Clair County and two in Livingston County) where between 1.5 percent and 2.2 percent of occupied homes did not have a heating source.
While Detroit wasn’t one of the roughly 55 communities in the region where all occupied homes had a heating source, about 0.6 percent of occupied homes in Detroit were without one. A closer look at the city though shows that up to 33 percent of the occupied homes in some census tracts were without a heating source. There were 27 census tracts throughout the city where between 3 and 33 percent of occupied homes were without a heating source. Seven of these census tracts were located along I-96. Additionally, there were two other clusters of occupied homes – just south of Hamtramck and Highland Park and in the downtown area – with the highest percentage of homes with no fuel source.
For those homes throughout the region that do have a heating source, utility gas was the most common source, followed by electricity.
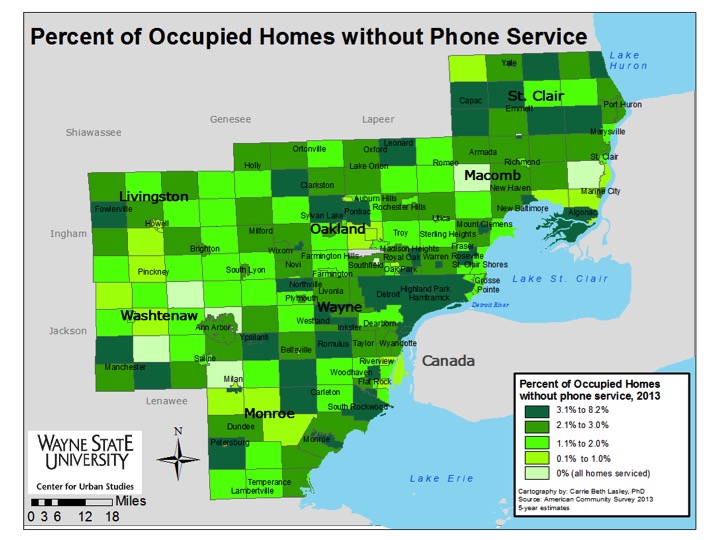
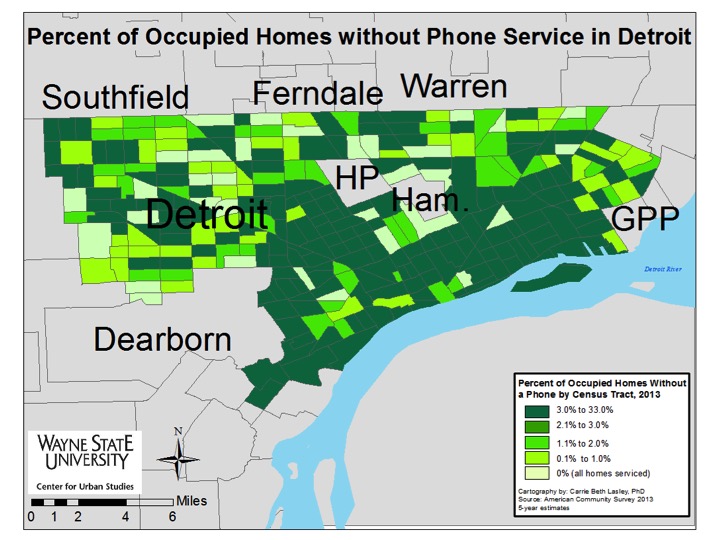
In 2013, up to 8.2 percent of occupied homes in Southeastern Michigan lacked any type of phone service (cell and/or landline), according to the American Community Survey. Those communities with the higher percentages of homes lacking phone service were primarily located in the more urban areas of the region, such as Detroit, Highland Park, and Pontiac, and the rural areas, such as several communities located throughout St. Clair, Livingston, and Monroe counties.
There were eight communities in the region where all occupied households had phone service. Four of these communities were located in Washtenaw County, two were located in Oakland County, one was in Macomb County, and another was in St. Clair County.
The city of Detroit was one of the 32 communities where between 3.1 and 8.2 percent of homes lacked phone service. In total, 4.8 percent of occupied homes in the city were without phone service. A drill down into the city shows that nearly half of the census tracts had between 3 and 33 percent of occupied homes without phone service.
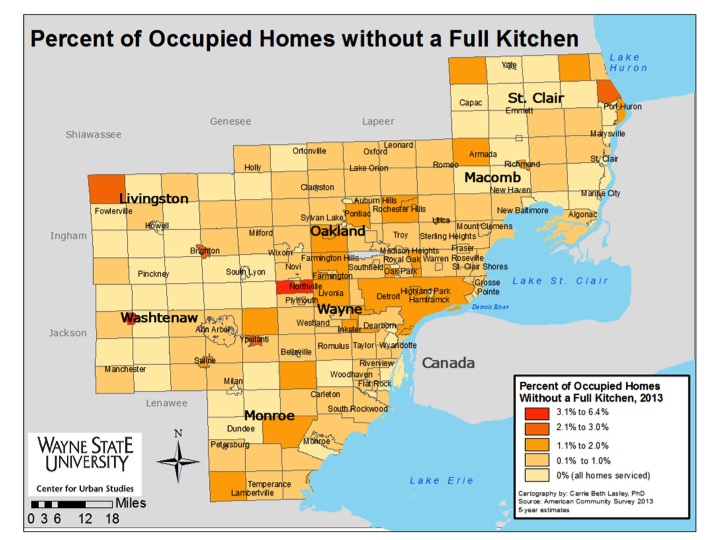
Northville Township and the city of Chelsea were the only two communities in the region where more than 3.1 percent of occupied homes did not have a full kitchen in 2013. In Chelsea, 5.6 percent of the homes were without a full kitchen and in Northville that number was 3.3 percent. According to the Census, having a full kitchen means having a sink with a faucet, a stove or a range and a refrigerator.
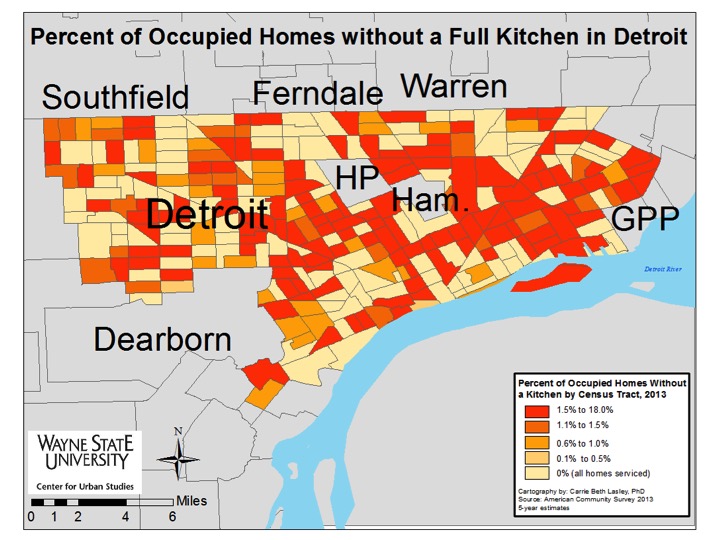
The city of Detroit was one of 22 communities where between 1.1 and 2 percent of homes were without a full kitchen. In Detroit, 1.7 percent of occupied homes were without a full kitchen. When looking at Detroit at the census tract level though we see that in more than 50 census tracts up to 18 percent of occupied homes were without a full kitchen.
While access to a full kitchen, whether it be lacking a stove or refrigerator or both, is a true day-to-day problem for many people, sometimes an occupied home lacks a full kitchen because it is in the process of being remodeled.